

| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website https://www.thejh.org |
Review
Volume 10, Number 2, April 2021, pages 41-45
Autoimmune Hemolytic Anemia Associated With Human Babesiosis
Pramuditha Rajapaksea, c, Kamila Bakirhanb
aDepartment of Internal Medicine, Danbury Hospital, Nuvance Health, Danbury, CT, USA
bDepartment of Hematology and Oncology, Danbury Hospital, Nuvance Health, Danbury, CT, USA
cCorresponding Author: Pramuditha Rajapakse, Department of Internal Medicine, Danbury Hospital, 24 Hospital Avenue, Danbury, CT 06810, USA
Manuscript submitted March 17, 2021, accepted March 31, 2021, published online April 27, 2021
Short title: AIHA Associated With Human Babesiosis
doi: https://doi.org/10.14740/jh820
| Abstract | ▴Top |
Babesiosis is characterized by non-autoimmune hemolytic anemia as a result of invasion of red blood cells by intraerythrocytic protozoans. Upon evaluation of patients who have ongoing hemolysis despite antibiotic treatment, a new entity of autoimmune hemolytic anemia (AIHA) was recently identified in some patients with babesiosis. The data are limited to case reports and one case series. The aim of this research was to synthetize data on this topic according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines using the PubMed database. In this review, we found that all patients who had developed AIHA were asplenic. All had Coombs test positive for IgG or both IgG and C3 indicating Warm AIHA. Some but not all required blood transfusion and plasma exchange. Majority of patients responded to steroids and had resolution of parasitemia on follow-up. We believe that this review will make the clinicians aware that babesiosis can not only cause non-immune hemolysis but also AIHA. It is important to differentiate between the two entities as antibiotics alone may not be sufficient for immune-mediated hemolysis caused by babesiosis.
Keywords: Autoimmune hemolytic anemia; Babesiosis; Hematology; Coombs positive
| Introduction | ▴Top |
Babesiosis is caused by intraerythrocytic protozoan of the genus Babesia, resulting in a febrile illness and a hemolytic anemia [1]. It is endemic in the Northeast and upper Midwest. The number of cases reported to the United States Centers for Disease Control and Prevention increased significantly over the last two decades, and babesiosis remains an emerging infectious disease (Fig. 1) [2-4].
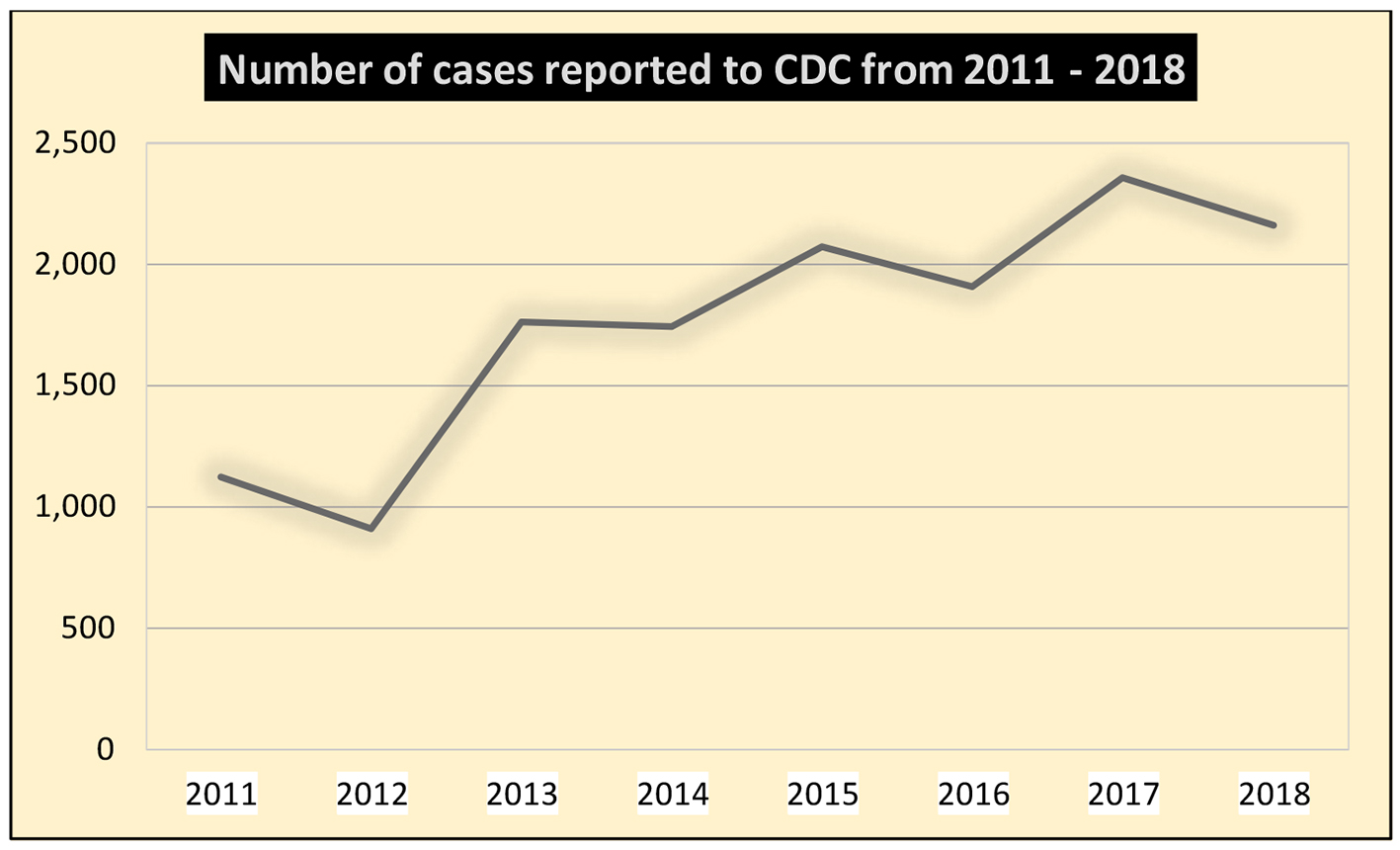 Click for large image | Figure 1. Increase in the number of reported cases of babesiosis in the Unites States since the disease became nationally notifiable in 2011 [4]. |
Anemia is one of the major laboratory findings of the illness [5, 6]. After the protozoans attach and enter the erythrocyte, they mature into trophozoites that undergo asexual budding to release daughter cells called merozoites. The merozoites released into the bloodstream invade nearby red blood cells. The intraerythrocytic protozoans invade other erythrocytes by disrupting the cell membrane, leading to non-immune-mediated hemolysis [7]. This process resolves with appropriate antimicrobial treatment and clearing of the parasitemia [6]. Autoimmune hemolytic anemia (AIHA), on the other hand, is caused by autoantibodies produced against the patient’s own erythrocytes, which leads to premature elimination of these cells from the circulation. This type of hemolysis is frequently seen in patients who have lymphoproliferative disorders or autoimmune conditions or who use certain medications [8]. AIHA is associated with certain infections, including HIV and malaria [9]. There have been sporadic cases and one case series reported of immune hemolysis complicating babesiosis in patients with ongoing parasitemia [10-13]. It is unclear if certain host factors may be associated with development of autoantibodies. It is possible that this complication was not recognized over last few decades despite high number of cases in endemic areas because the prevalence of asplenia is very low and non-autoimmune hemolysis can mask concurrent autoantibody-mediated hemolysis.
However, no systematic reviews have been performed to characterize these patients to the best of our knowledge. In this review, we have described the clinical features, laboratory findings, associated factors and the management of patients with AIHA in the setting of Babesia microti (B. microti) infection. We have also reviewed their medical history to identify potential risk factors associated with AIHA. Subsequently, the review will help clinicians to identify this under-recognized cause of anemia in human babesiosis and treat accordingly.
| Materials and Methods | ▴Top |
Database and the keywords
A systematic review of the literature following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines was performed using the PubMed database for case reports and case series of B. microti infection with AIHA from the date of database inception to February 2021. The following keywords alone and/or in combination were used: “babesiosis AND warm antibody mediated autoimmune hemolytic anemia,” “Babesia microti AND autoantibodies”.
Definitions
We defined AIHA as antibody-mediated direct antigen test (DAT) positive (also known as Coombs positive) hemolysis leading to anemia not due to another cause such as a hemolytic transfusion reaction or paroxysmal nocturnal hemoglobinuria (PNH) as described in case reports. Evidence of hemolysis includes increased reticulocyte count that is not due to active bleeding, recent correction of iron deficiency or nutritional anemia, or erythropoietin administration; spherocytosis; low haptoglobin; high lactate dehydrogenase (LDH) and indirect (unconjugated) bilirubin. Patients with hemoglobinopathies such as thalassemia or sickle cell disease; enzymopathies such as glucose 6 phosphate dehydrogenase (G6PD) or pyruvate kinase (PK) deficiency; and membrane defects such as hereditary spherocytosis, elliptocytosis, or stomatocytosis were included if they have no prior history of DAT positive hemolytic anemia. Diagnosis of babesiosis was defined by a positive babesiosis polymerase chain reaction (PCR) and/or presence of babesia parasites in peripheral blood smear.
Selection criteria
We selected only definite cases of B. microti infection diagnosed by PCR and/or peripheral blood smear. Duplicate articles, narrative reviews and cases of babesiosis without AIHA were excluded. The flowchart of selection of the final cases included in our analysis is illustrated in Figure 2.
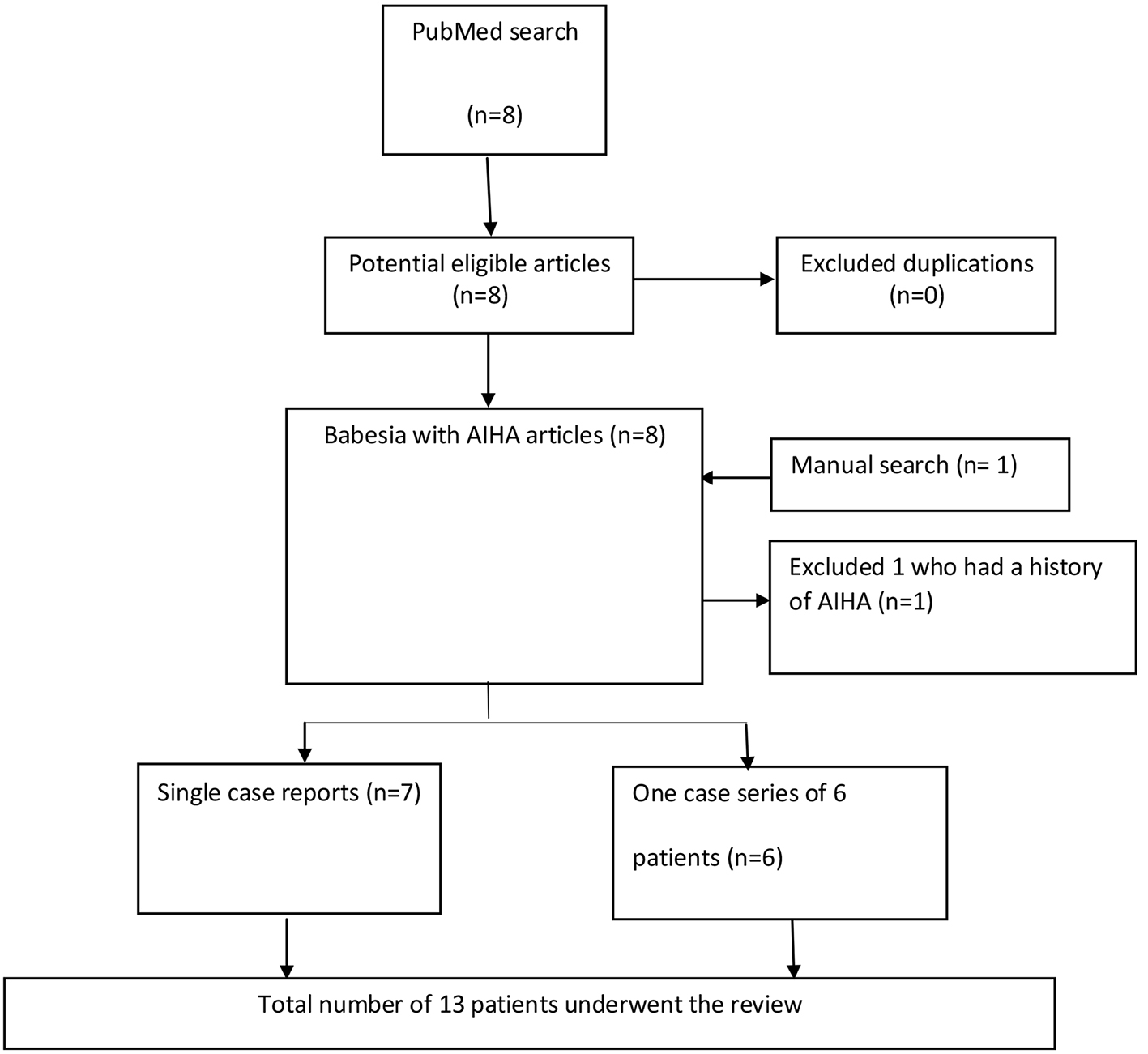 Click for large image | Figure 2. The flowchart delineates methodology and literature selection process according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses. |
Data collection
Two researchers independently and blindly identified and selected the titles, abstracts and full texts obtained in the database search. Discrepancies of the selected articles were resolved by consensus. After completing the PubMed PRISMA search, we completed a manual search by subsequently screening the reference lists of all selected articles. An excel table was constructed, and for each case, we collected patient demographics, clinical presentation, medical comorbidities, vital signs on admission, time from presentation to diagnosis, patient’s immune status, presence of co-infection, laboratory values (hemoglobin, reticulocyte count, DAT test results, level of parasitemia, babesiosis PCR results, etc.) treatment and clinical outcome on follow-up. Of 13 cases reported, seven cases were collected from single case reports; there was one case series including six cases from a single institution [10-13].
| Results | ▴Top |
A total of 13 cases constituted the final sample (Supplementary Material 1, www.thejh.org). All reported cases in this review were from different endemic regions in the USA (NY, MA and PA) except one patient who was from Maryland with no clear documentation on travel history. The age distribution was broad. The youngest patient was 11 years old, and the oldest was 84 years old. Although advanced age is a risk factor for majority of other babesiosis-related complications (such as splenic rupture, acute respiratory distress syndrome and acute kidney injury), the risk for autoimmune hemolysis appears to be more related to comorbidities (asplenia, sickle cell anemia and malignancy) rather than age. Eight cases were male and five were female. Although male predominance has been described in splenic complications of babesiosis, AIHA appears to occur in both males and females; however, this sample size is insufficient to make conclusions. One of the most interesting findings was that all the 13 patients were asplenic. The cause for splenectomy was sickle cell disease (SCD) in two patients. One case had history of autoimmune disease, two had hematologic malignancies and two had other solid tumors (gastric cancer and metastatic neuroendocrine tumor of the pancreas). Surprisingly, three of the cases had acquired babesiosis because of a blood transfusion with retrospective screening of the received blood being positive for babesia in all three.
Comorbidities and immune status
All patients had different underlying comorbidities which increased their risk not only for severe disease but also for antibody-mediated hemolysis. The two young patients were asplenic in the setting of SCD. Middle-aged patients had a history of autoimmune disease making them more susceptible to auto-antibody production in the background of infection. The elderly patients were noted to have hematologic malignancies or solid tumors and thus fall into the immunocompromised group who are at high risk of severe disease.
Clinical manifestation and co-infection
The most frequently reported symptom in this cohort of patients was fever (7/13, 53.8%) and the most common examination finding was jaundice (4/13, 30.8%). All patients required in-patient level of care. Co-infection with other tick-borne illness was only documented in one case. It is unclear if presence of co-infection with another tick-borne illness affects the risk of AIHA.
Laboratory findings
Babesiosis was confirmed by peripheral blood smear or PCR in all patients. All had positive DAT for either IgG alone or both IgG and C3 indicating that this process is warm AIHA. The B. microti parasitemia level ranged from 2.5% to > 30%. One had ongoing hemolysis despite the clearance of parasitemia. Parasitemia level usually correlates with the severity of illness in babesiosis, with parasitemia level > 10% considered to be severe infection [7]. It is interesting to note that two patients had clinically severe AIHA requiring packed red blood cell (PRBC) transfusions despite a very low level of parasitemia (< 1% and 3.9%). However, larger cohorts should be examined to identify an association. The reported hemoglobin (Hgb) levels ranged between 5.2 to 10.9 g/dL. The case series of six only recorded the hematocrit which ranged between 18% and 24%. Other hematologic complications such as splenic rupture are known to be associated with a low Hgb. However, such association has not been evaluated in patients with AIHA. Thrombocytopenia was reported in four out of the 13 patients. Among them, one patient was initially diagnosed with Evans syndrome and on evaluation was found to have babesiosis. Thrombocytosis was seen in six. Platelet count was not available in three. The reticulocyte percentage ranged between 1% and 17%.
Treatment and outcome
The severity of AIHA varied, as did the medical management of the condition. All patients required in-patient level of care and were treated with azithromycin and atovaquone. Two cases required exchange transfusion and six (46.2%) required PRBC transfusions during the episode of anemia. Seven cases (53.8%) were given steroids for AIHA. Four patients had AIHA during parasitemia and seven had a late onset: 1 to 4 weeks later once parasitemia had resolved. One patient presented late; 4 weeks after symptom onset and at presentation, the patient was diagnosed with babesiosis and AIHA at the same time. In one patient, the duration from babesiosis diagnosis to development AIHA was not documented. In this review, two patients died from ongoing hemolysis which corresponded to a mortality rate of 15.4%. One of them was 44 years old, and had a very high parasitemia > 30%. He died from severe hemolysis refractory to multiple PRBC transfusions and therapeutic apheresis. Additionally, he was diagnosed late as babesiosis was incidentally found during a hospitalization for pancreatitis and this emphasizes the importance of timely diagnosis to decrease morbidity and mortality. All patients received antimicrobials although in many of them the duration of therapy was not documented. All except three were started on azithromycin and atovaquone. One patient received clindamycin and quinine in 1993 as it was the first successful antimicrobial regimen before azithromycin and atovaquone became the treatment of choice. Currently, the preferred regimen consists of oral azithromycin plus atovaquone; clindamycin plus quinine is an alternative option [6, 7]. Two patients were initially started on clindamycin and quinine and due to suboptimal response, they were switched to azithromycin and atovaquone.
| Discussion | ▴Top |
Upon our review, two different patterns were identified in the development of AIHA-associated babesiosis. Majority had auto-antibodies against red blood cells 1 to 4 weeks after the illness when parasitemia had resolved (69.2%). Others had auto-antibody-mediated hemolysis concurrently with parasitemia (30.8%). No alternative explanations for AIHA were found in all the patients. Although Hodgkin’s lymphoma and acute myeloid leukemia are rarely associated with AIHA, both the patients with these cancers were in remission at the time of presentation. In one patient who had received a transfusion in the 26 days before presentation, DAT was negative 10 months prior to detection of parasitemia. AIHA has not been associated with atovaquone, azithromycin, or clindamycin and thus drug-induced AIHA was unlikely. Although quinine is a known drug to cause AIHA, quinone was prescribed after detection of DAT + AIHA in all four patients who received quinine.
The pathogenesis of AIHA in babesiosis is unclear. It is believed that this may have similar pathogenesis to immune-mediated hemolysis observed in malaria [14]. Immune complex-mediated, or type III hypersensitivity is one possible explanation. Excess production of immunoglobulins in response to foreign antigens causes formation of immune complexes. In asplenic patients, these are not cleared efficiently by phagocytosis and thus get accumulated, leading to activation of classical complement cascade resulting in lysis of red cells [15]. Cross-reacting antibodies initially elicited against B. microti antigens, and subsequently act against human antigens. Asplenic patients are at higher risk due to poor clearance of the surface antigens on RBCs. This could potentially explain the late onset AIHA after resolution of parasitemia observed in eight out of the 13 patients.
Our study has several limitations. We reviewed the cases that were only published in journals that are indexed in the PubMed. Additionally, we have not reviewed cases published in languages other than English which contributes to publication bias.
| Conclusion | ▴Top |
AIHA is an emerging hematologic complication of babesiosis, particularly among asplenic patients. This is often under-recognized due to limitation of cases to endemic areas and the low prevalence of asplenia. If patients with babesiosis continue to have hemolysis despite standard treatment, we suggest evaluating them for AIHA. It is important to differentiate non-autoimmune hemolysis from autoimmune hemolysis as the approach to treatment is different. AIHA in the setting of babesiosis has shown a positive response to both intravenous and oral steroids.
| Supplementary Material | ▴Top |
Suppl 1. Characteristics of Patients Who Had AIHA in the Setting of Babesiosis.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Author Contributions
Study conception and design: PR; data collection: PR and KB; analysis and interpretation of results: PR and KB; draft manuscript preparation: PR and KB. All authors reviewed the results and approved the final version of the manuscript.
Data Availability
The data that support the findings of this study is available from the corresponding author upon reasonable request.
| References | ▴Top |
- Vannier E, Krause PJ. Human babesiosis. N Engl J Med. 2012;366(25):2397-2407.
doi pubmed - Gray EB, Herwaldt BL. Babesiosis Surveillance - United States, 2011-2015. MMWR Surveill Summ. 2019;68(6):1-11.
doi pubmed - Krause PJ, McKay K, Gadbaw J, Christianson D, Closter L, Lepore T, Telford SR, 3rd, et al. Increasing health burden of human babesiosis in endemic sites. Am J Trop Med Hyg. 2003;68(4):431-436.
doi pubmed - Centers for Disease Control and Prevention, (CDC). Babesiosis surveillance - 18 States, 2011. MMWR Morb Mortal Wkly Rep. 2012;61(27):505-509.
- Reubush TK, 2nd, Cassaday PB, Marsh HJ, Lisker SA, Voorhees DB, Mahoney EB, Healy GR. Human babesiosis on Nantucket Island. Clinical features. Ann Intern Med. 1977;86(1):6-9.
doi pubmed - Sanchez E, Vannier E, Wormser GP, Hu LT. Diagnosis, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: a review. JAMA. 2016;315(16):1767-1777.
doi pubmed - Vannier EG, Diuk-Wasser MA, Ben Mamoun C, Krause PJ. Babesiosis. Infect Dis Clin North Am. 2015;29(2):357-370.
doi pubmed - Brodsky RA. Warm autoimmune hemolytic anemia. N Engl J Med. 2019;381(7):647-654.
doi pubmed - Hill A, Hill QA. Autoimmune hemolytic anemia. Hematology Am Soc Hematol Educ Program. 2018;2018(1):382-389.
doi pubmed - Narurkar R, Mamorska-Dyga A, Nelson JC, Liu D. Autoimmune hemolytic anemia associated with babesiosis. Biomark Res. 2017;5:14.
doi pubmed - Santos MA, Tierney LM, Jr., Manesh R. Babesiosis-associated warm autoimmune hemolytic anemia. J Gen Intern Med. 2020;35(3):928-929.
doi pubmed - Woolley AE, Montgomery MW, Savage WJ, Achebe MO, Dunford K, Villeda S, Maguire JH, et al. Post-babesiosis warm autoimmune hemolytic anemia. N Engl J Med. 2017;376(10):939-946.
doi pubmed - Karkoska K, Louie J, Appiah-Kubi AO, Wolfe L, Rubin L, Rajan S, Aygun B. Transfusion-transmitted babesiosis leading to severe hemolysis in two patients with sickle cell anemia. Pediatr Blood Cancer. 2018;65(1):e26734.
doi pubmed - Rivera-Correa J, Rodriguez A. Autoimmune anemia in Malaria. Trends Parasitol. 2020;36(2):91-97.
doi pubmed - Warrington R, Watson W, Kim HL, Antonetti FR. An introduction to immunology and immunopathology. Allergy Asthma Clin Immunol. 2011;7(Suppl 1):S1.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Hematology is published by Elmer Press Inc.