


| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website http://www.thejh.org |
Case Report
Volume 1, Number 4-5, October 2012, pages 100-101
Aplastic Anemia in a Patient With Wilson's Disease
Sanjeev Kumar Sharmaa, d, Avinash Kumar Singha, Pawan Kumar Singha, Tulika Setha, Pravas Mishraa, M Vanathib, Mom Dasc, Manoranjan Mahapatraa, Haraprasad Patia
aDepartment of Hematology, All India Institute of Medical Sciences, New Delhi, India
bDepartment of Ophthalmology, All India Institute of Medical Sciences, New Delhi, India
cDepartment of Ophthalmology, Perfect Wellness Clinic, Malviya Nagar, New Delhi, India
dCorresponding author: Sanjeev Kumar Sharma, Department of Hematology, All India Institute of Medical Sciences, New Delhi, India
Manuscript accepted for publication August 13, 2012
Short title: Wilson's Disease and Aplastic Anemia
doi: https://doi.org/10.4021/jh39e
| Abstract | ▴Top |
An 8-years-old boy was admitted with jaundice and weakness. Workup for jaundice revealed the diagnosis of Wilson's disease. Patient had pancytopenia and bone marrow biopsy showed hypocellular marrow suggestive of aplastic anemia. This case represents an unusual association of Wilson's disease with aplastic anemia. Treatment with zinc decreased the bilirubin levels but cytopenias persisted.
Keywords: Wilson's disease; Aplastic anaemia; Copper
| Introduction | ▴Top |
Wilson's disease (hepatolenticular degeneration) is an autosomal recessive defect in cellular transport of copper with prevalence of approximately 1 in 30,000 live births [1]. Clinical manifestations arise because of hepatic and extrahepatic deposition of copper. Tissue copper deposition can occur in various organs, leading to hepatic, neurologic, hematologic, and renal impairment [2, 3]. The hepatic injury is probably caused by excess copper which acts as a pro-oxidant and promotes the attack by free radicals. Treatment is aimed at removing excess copper and preventing its re-accumulation. Acquired aplastic anemia is due to bone marrow failure, and its etiology is unknown in most of the cases. Hemolysis has been reported in patients with Wilson's disease but aplastic anemia is an unreported finding. Our patient presented simultaneously with manifestations of Wilson's disease and aplastic anemia.
| Case Report | ▴Top |
An 8-years-old boy was admitted with progressively increasing jaundice and weakness for 3 months. There was no history of fever or bleeding from any site. Clinically, he was pale and icteric without any lymphadenopathy and hepatosplenomegaly. His haemogram revealed pancytopenia with haemoglobin 77 g/L, total leukocyte count 1.9 × 109/L, platelet count 20 × 109/L, absolute neutrophil count 0.1 × 109/L and reticulocyte count 0.01%. His total bilirubin was 26.1 mg/dL with conjugated bilirubin of 23.1 mg/dL and alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase and gamma glutamyl transpeptidase were 1362/902/117/46 IU/L respectively. Investigations were negative for viral hepatitis including hepatitis A, E, B and C. Serology for parvovirus-B19, cytomegalovirus, varicella zoster and leptospira were negative. Serum ceruloplasmin levels were reduced, 2.5 mg/dL (normal 18 - 50 mg/dL) and 24-hours urinary copper levels were raised, 120 µg/24 hrs (normal 20 -50 µg/24 hrs). Slit lamp examination of the eye revealed the presence of Kayser-Fleischer rings (Fig. 1, 2), which are brownish rings that represent fine pigmented granular deposits of copper in Descemet's membrane in the cornea. Bone marrow biopsy showed cellularity of less than 5% (Fig. 3). Chromosomal breakage study did not show increased chromosomal fragility with mitomycin-C. He was diagnosed as a case of Wilson's disease with very severe aplastic anemia and was treated with zinc sulphate 50 mg twice daily along with supportive treatment for cytopenias.
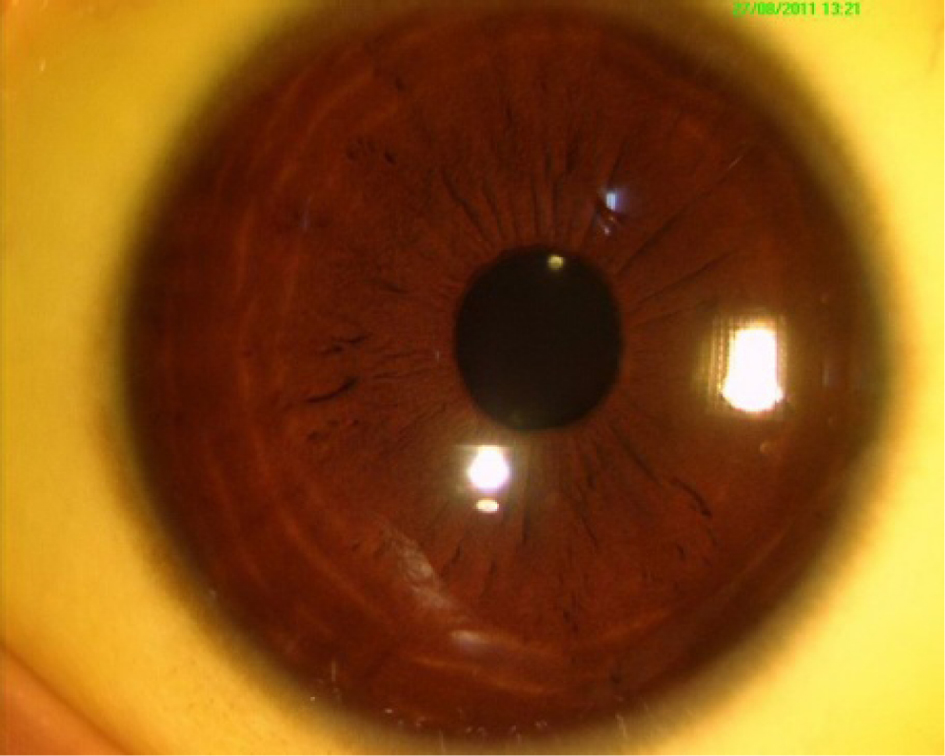 Click for large image | Figure 1. KF ring in a patient with Wilson's disease. |
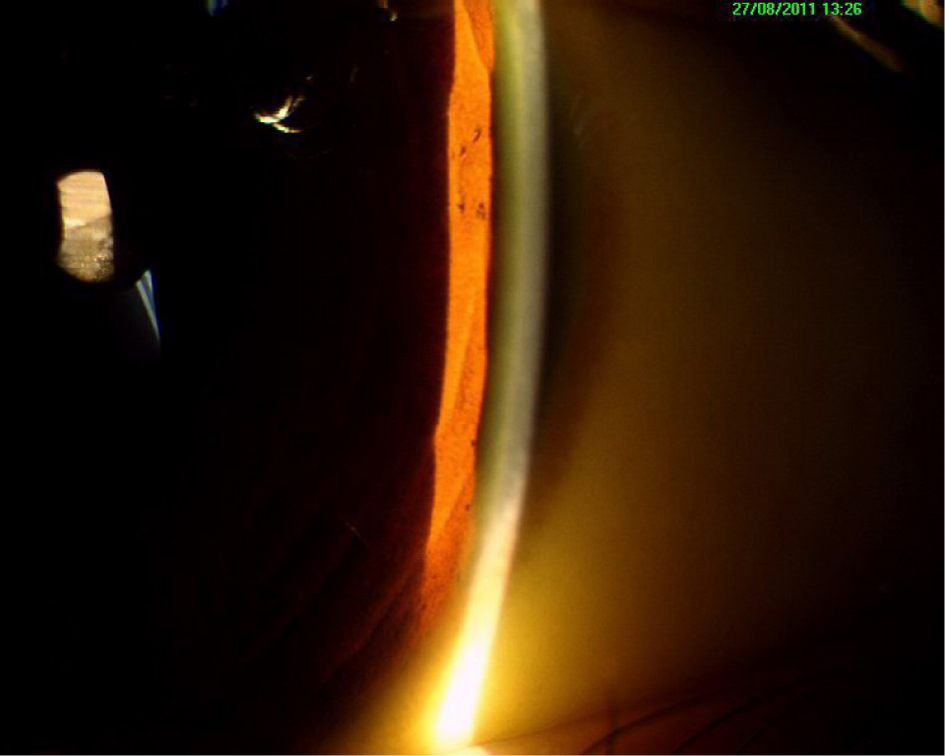 Click for large image | Figure 2. Slit lamp examination of eye showing KF ring. |
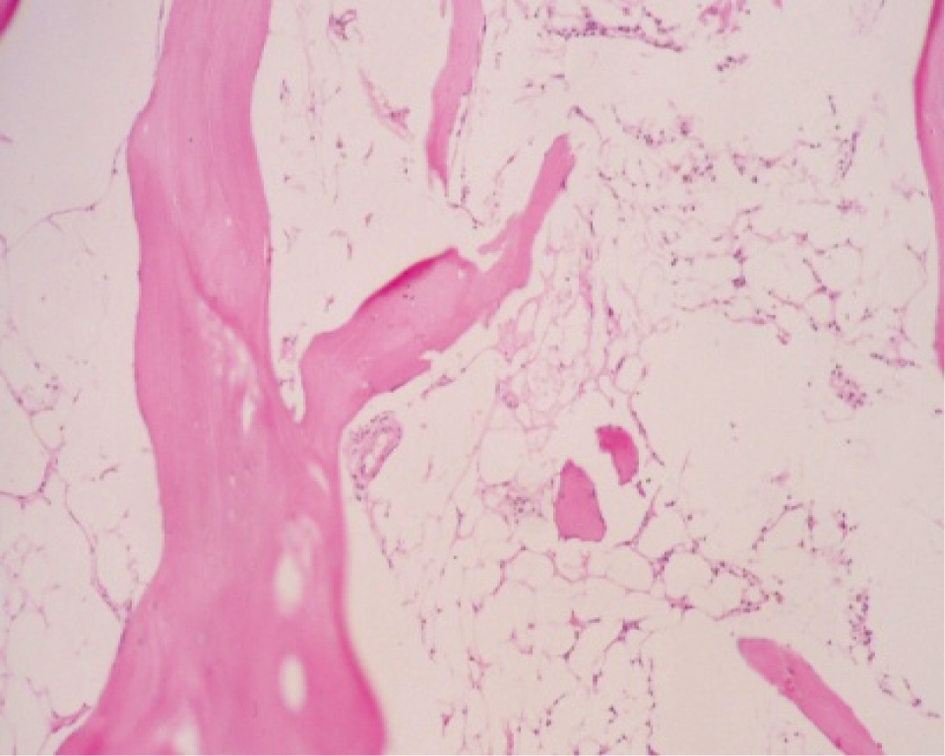 Click for large image | Figure 3. Bone marrow biopsy of the patient showing hypocellular marrow (40 ×). |
| Discussion | ▴Top |
Wilson's disease is an autosomal recessive disorder resulting in defective cellular copper transport [1]. Clinical manifestations arise as hepatic and extrahepatic copper deposition progresses. They are rare before age 6 and almost always present before the age of 30 years. A very low serum ceruloplasmin level (< 5 mg/dL) provides strong evidence for the diagnosis of Wilson's disease [2, 3]. The earliest lesion in Wilson's disease occurs in the liver, the site of initial copper accumulation. Kayser-Fleischer rings are characteristic feature of Wilson's disease. They are usually detected by slit-lamp examination but may be clinically visible in some cases. KF rings are seen in 50-60% of patients who present with hepatic involvement. About 5 to 10% of patients with Wilson's disease can have haemolytic anemia [3, 4].
Copper deficiency and treatment with penicillamine, a copper chelator, used in the treatment of Wilson's disease has been reported to cause cytopenias including aplastic anemia [5, 6], but aplastic anemia, per se in Wilson's disease is an unreported finding. Aplastic anemia is characterized by diminished or absent hematopoietic precursors in the bone marrow, often due to injury to the pluripotent stem cell. Management of our case was challenging as this was probably the first reported case of Wilson's disease presenting as aplastic anemia. He was not given penicillamine because he had cytopenias, and treatment with zinc sulphate resulted in reduction in bilirubin to 6mg/dl, without any improvement in the cytopenias. He developed febrile neutropenia and died of pneumonia before any definite management of aplastic anemia could be done.
Conflict of Interest
The authors declare no conflicts of interest.
| References | ▴Top |
- Brewer GJ. Autonomic dysfunction in Wilson's disease. Clin Auton Res. 2002;12(3):139-140.
pubmed doi - Steindl P, Ferenci P, Dienes HP, Grimm G, Pabinger I, Madl C, Maier-Dobersberger T, et al. Wilson's disease in patients presenting with liver disease: a diagnostic challenge. Gastroenterology. 1997;113(1):212-218.
pubmed doi - Gow PJ, Smallwood RA, Angus PW, Smith AL, Wall AJ, Sewell RB. Diagnosis of Wilson's disease: an experience over three decades. Gut. 2000;46(3):415-419.
pubmed doi - Stremmel W, Meyerrose KW, Niederau C, Hefter H, Kreuzpaintner G, Strohmeyer G. Wilson disease: clinical presentation, treatment, and survival. Ann Intern Med. 1991;115(9):720-726.
pubmed - Haddad AS, Subbiah V, Lichtin AE, Theil KS, Maciejewski JP. Hypocupremia and bone marrow failure. Haematologica. 2008;93(1):e1-5.
pubmed doi - Wiggelinkhuizen M, Tilanus ME, Bollen CW, Houwen RH. Systematic review: clinical efficacy of chelator agents and zinc in the initial treatment of Wilson disease. Aliment Pharmacol Ther. 2009;29(9):947-958.
pubmed doi
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Hematology is published by Elmer Press Inc.