Figures
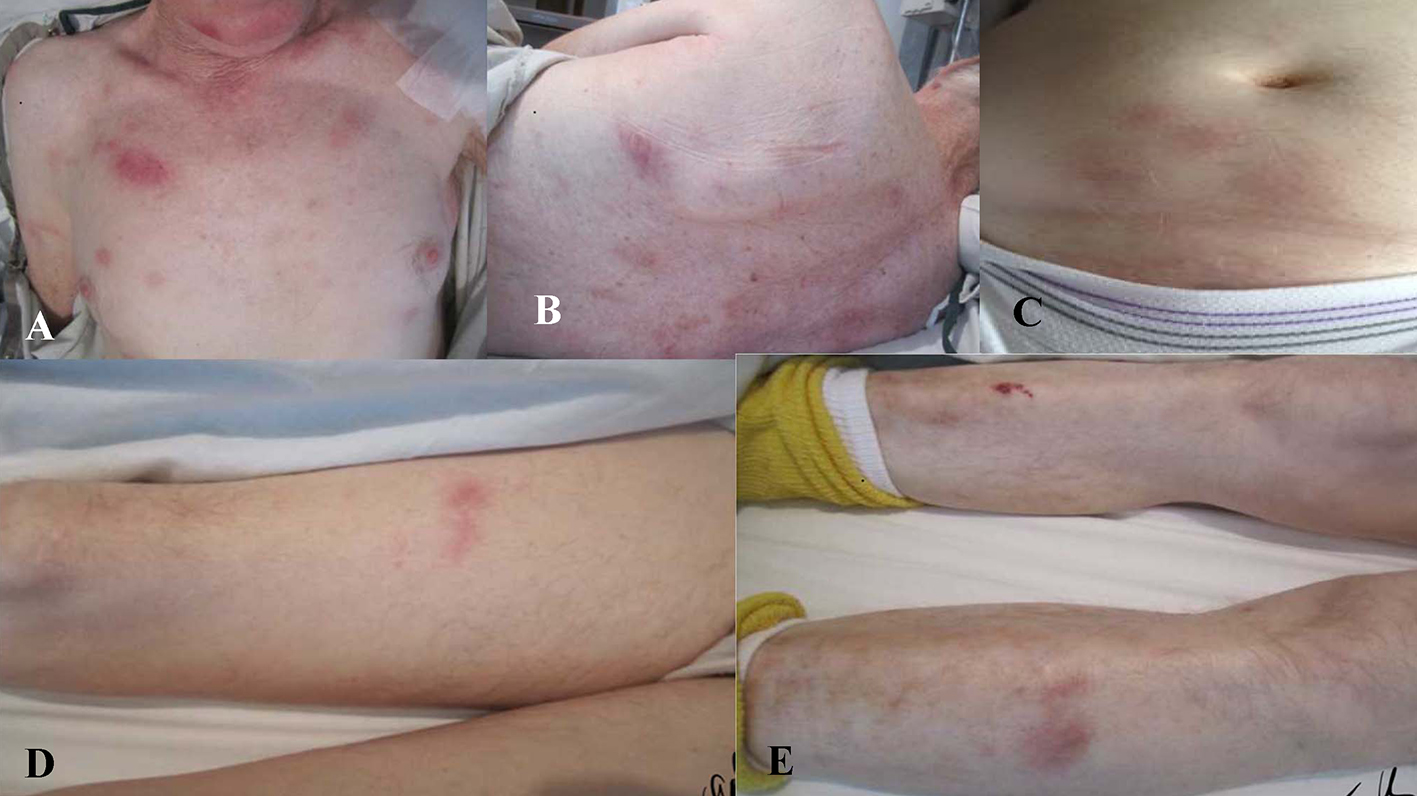
Figure 1. Mildly tender, indurated, dull red, subcutaneous nodules present on (A) chest, (B) trunk, (C) abdomen, and (D, E) extremities.
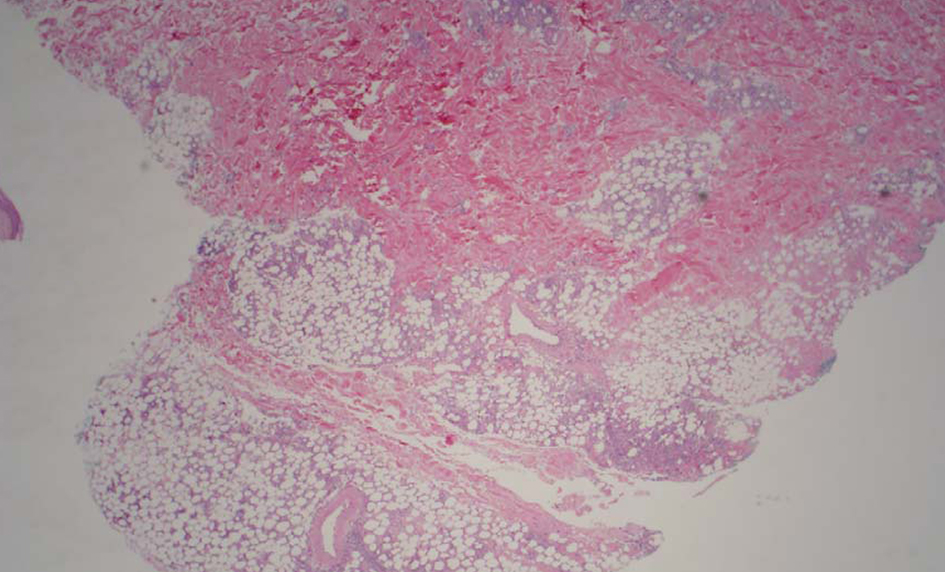
Figure 2. Low power image shows moderate subcutaneous inflammation localized to the lobules (lobular panniculitis).
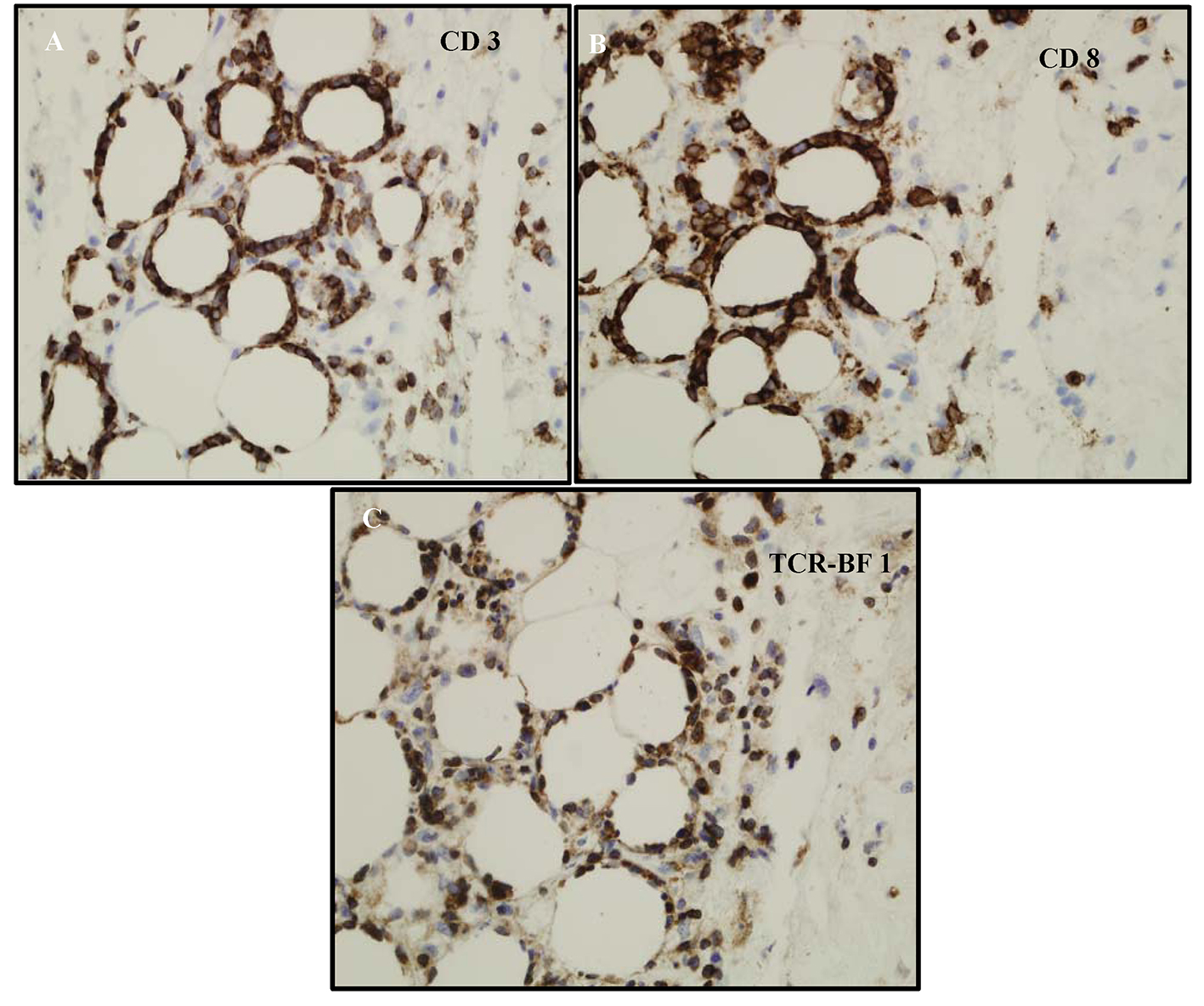
Figure 3. (A) CD3 labels the lymphocytes-supporting T cells. (B) Phenotype of the cells ends up being CD3+, CD8+, CD4-, CD56-, and TCR-BF1 positive. It appears to be mature T-cell phenotype with CD8 and derived from alpha/beta T-cells not gamma/delta. (C) The atypical lymphocytes appear to label with TCR-BF1 immunohistochemical study in keeping with an alpha beta T-cell, rather than a gamma delta T-cell origin.
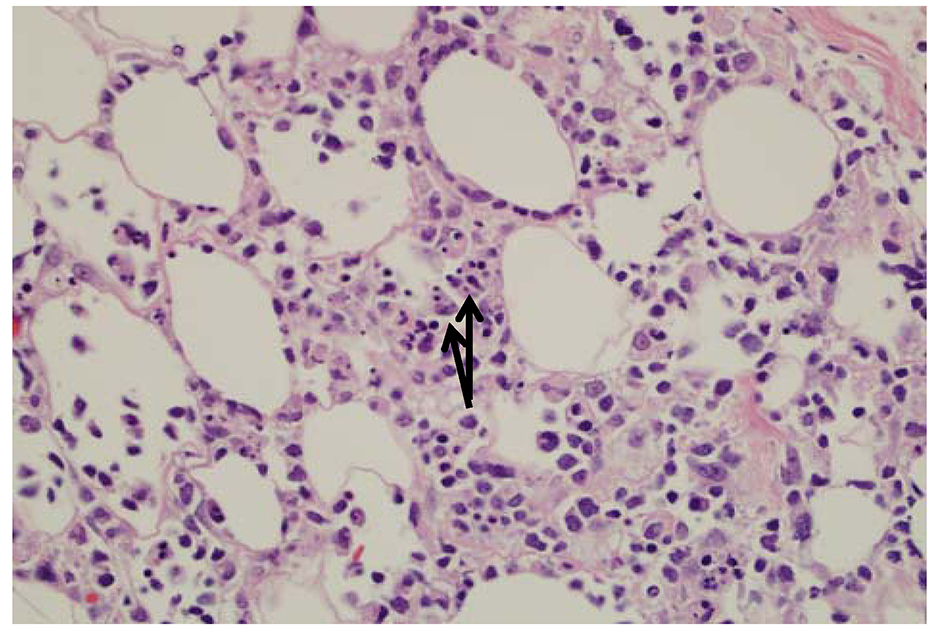
Figure 4. The fat is involved by an atypical lymphoid infiltrate with rimming of atypical lymphocytes around adipocytes. There are occasional histiocytes that engulf the lymphocytes, so called “bean bag” cells by arrows.
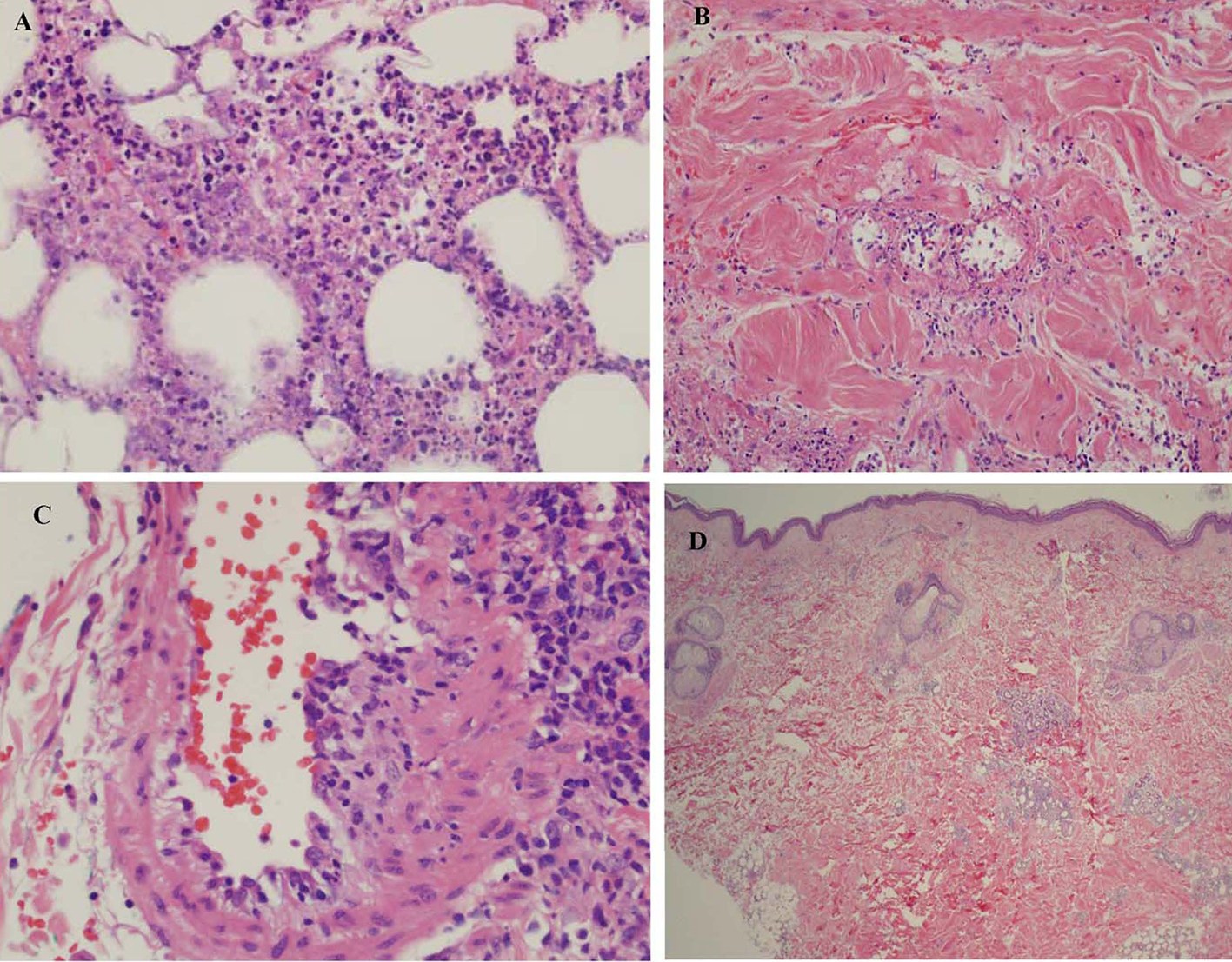
Figure 5. (A) Subcutaneous fat showing extensive necrotizing panniculitis with predominantly neutrophilic inflammation. (B) There is evidence of vasculitis within the subcutaneous septa. (C) A medium sized blood vessel shows some neutrophilic inflammation. (D) Biopsy shows less inflammation involving the subcutis and no extensive necrosis or vasculitis.