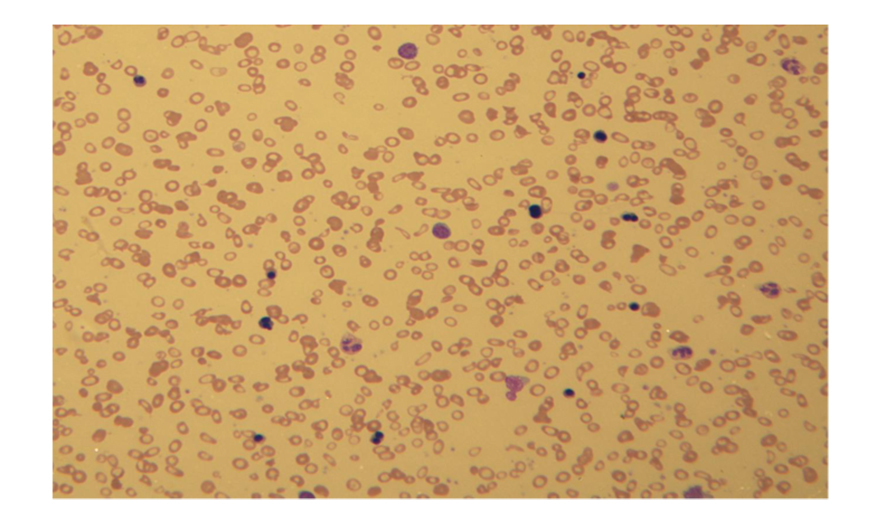
Figure 1. Severe microcytic, hypochromic anemia with marked poikilocytosis and numerous nucleated red blood cells with dysplastic changes including bi-nucleation.
| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website http://www.thejh.org |
Case Report
Volume 3, Number 1, March 2014, pages 13-18
Erythroblastic Synartesis in a Patient With Low Grade B Cell Lymphoma
Figures
Table
| Author | Year | Age | sex | Hgb | M -protein | Other Labs | Underlying disease | Therapy | Long term Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Abbreviations: ACLA: anti cardiolipin antibody; AN A: antineutrophil antibodies; CLL: chronic lymphocytic leukemia; ESR: erythrocyte sedimentation rate; F: female; Hgb: hemoglobin; LDH: lactate dehydrogenase; M: Male; NR: not reported; OSH: outside hospital; Plt: platelets; ppx: prophylactic; T-bili: total bilirubin; TD: transfusion dependent; WBC: white blood cell count. | |||||||||
| Gorius [1] | 1973 | 74 | F | 7.75 (Transfusion dependent) | NR | Serum iron 105, TIBC 240, T bili 1.3, Coombs negative, Retic count 0.5%, Negative HAM’s test, no agglutination with anti-i. | NR | NR | NR |
| Nagao [3] | 1976 | 29 | F | NR | NR | Hematocrit 24%, Plt 263 × 104/cm2, WBC 5,900/cm2, retic count < 1‰ | NR | NR | NR |
| Cramer [4] | 1999 | 24 | F | 6 | NR | Reticulocyte count reduced; nl serum iron; | Small lymphocytic lymphoma | Chlorambucil → no response; corticosteroids → decreased transfusion requirements, anemia recurred with taper; multiagent chemotherapy → hgb stabilized | Died from Richter transformation after 10 years. |
| 70 | F | 5.5 | IgG, kappa 3 g/L | Iron 35, ferritin 175, LDH 667, bilirubin 9.3, haptoglobin markedly reduced, Retic count 20 × 109/L Coombs positive for complement, lupus anticoagulant present, ACLA positive | Sjogren’s syndrome | Corticosteroids with resolution of anemia, but relapse with withdrawal of steroids | NR | ||
| 46 | F | 7.9 | IgG, kappa (1.7 g/L) | WBC 18.7 with 76% lymphs, | CLL | 6 cycles low dose CHOP, ppx IVIG, 1 year chlorambucil → remission (hgb 12.7); relapsed 6 months later with hgb 6.9; fludarabine 6 mo later with transient incomplete remission | Died from septic cellulitis 3 years later | ||
| Bacher [6] | 2004 | 74 | M | 9 | IgG, kappa (3.3 g/dL) | ESR 75, ANA neg, AMA neg, C4 < 0.01, C3 0.52 (low), IgG 35.4 (elevated), No signs of hemolysis, Retic count 15‰. | None | None (In good clinical condition) | NR |
| Liapis [7] | 2008 | 70 | NR | 4.9 | IgG, kappa (1.5 g/L) | Reticulocyte count 1.5 × 109/L; ferritin, B12, and folate nl. | Small lymphocytic lymphoma | Therapy (not specified) of small lymphoctic lymphoma lead to resolution | NR |
| Zaninoni [5] | 2010 | 44 | M | 9 | NR | Reduced reticulocytes (20 × 109/L), unconjugated bili 1.8, LDH 550, haptoglobin < 20, DAT negative | NR | Steroids and cyclosporine “with some response” at OSH; Repeat prednisone with clinical response. Relapsed 2 years later and again treated with prednisone taper with good response. | NR |
| Papakonstantinou [8] | 2010 | 35 | M | 8.1 (Transfusion dependent) | None | WBC 2.8 (29% PMN, 53% lymphocytes), retic count 105.2 × 109 L; LDH 355, IgA undetectable, CD19+ B-lymphocytes reduced (21 × 106/L); no monoclonal B-cell population detected. Serum IgG, IgM, haptoglobin, vitamin B12, folic acid, ferritin, and B2-microglobulin were normal. Coombs negative. | None | Prednisolone with no response, IVIG with no response; complete remission with rituximab | Response maintained at 30 months. |