










| Journal of Hematology, ISSN 1927-1212 print, 1927-1220 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Hematol and Elmer Press Inc |
| Journal website http://www.thejh.org |
Case Report
Volume 1, Number 4-5, October 2012, pages 105-107
Sacroiliac Joint Involvement in A Patient With Hemophilia A: Case Report
Ozcan Hiza, e, Levent Ediza, Fahrettin Demirdagb, Yasemin Ozkana, Ramazan Esenc, Savas Gunerd
aPhysical Medicine and Rehabilitation Department, Yuzuncu Yil University Medical Faculty, Van, Turkey
bPhysical Medicine and Rehabilitation Department, Elazig State Hospital, Elazig, Turkey
cHaematology Department, Yuzuncu Yil University Medical Faculty, Van, Turkey
dOrthopaedics and Traumatology Department, Yuzuncu Yil University Medical Faculty, Van, Turkey
eCorresponding author: Ozcan Hiz, Yuzuncu Yil University Medical Faculty Physical Medicine and Rehabilitation Department, Van, Turkey
Manuscript accepted for publication September 14, 2012
Short title: Sacroiliac Involvement in Hemophilia
doi: https://doi.org/10.4021/jh43e
| Abstract | ▴Top |
Hemophilic arthropathy is characterized by chronic proliferative synovitis and cartilage destruction as a result of recurrent intra-articular bleeding. Hemophilic arthropathy can be seen in many joints such as knee, shoulder, hip and ankle. However, the information related to the sacroiliac joint involvement was not found in the accessible literature and electronic medium. In this article, unilateral sacroiliac joint involvement is presented in a patient with hemophilia for 15 years who developed severe destruction in bilateral knees and admitted to our outpatient clinic because of pain over hip region.
Keywords: Hemophilia A; Sacroiliac joint; Osteoarthritis
| Introduction | ▴Top |
Hemophilia is a rare hereditary disease which is developed most commonly due to deficiency of factor VIII (hemophilia A) and factor IX (hemophilia B or Christmas disease) and characterized by bleeding disorders. It is usually inherited by X-linked recessive type and exceptions, is seen in males. In rare cases, some spontaneous mutations may occur. The disease is examined in three categories due to lack of circulating clotting factors in the blood; severe (< 1%), moderate (1-5%), mild (> 5%). Hemophilic arthropathy is characterized by chronic proliferative synovitis and cartilage destruction as a result of recurrent intra-articular bleeding. Hemophilic arthropathy can be seen in many joints such as knee, shoulder, hip and ankle [1, 2]. However, the information related to the sacroiliac joint involvement was not found in the accessible literature and electronic medium. In this paper, we presented arthropathy in both knees and right sacroiliac joint involvement in a patient diagnosed with hemophilia A.
| Case Report | ▴Top |
Twenty-five-year-old male patient with moderate to severe hemophilia A (factor VIII, c: 1% -5%) was negative for the level of the inhibitory factor. Knee arthropathy had developed as a result of recurrent knee joint hemorrhages for 15 years. During this period, severe left knee extension deformity developed and the patient had become unable to do knee flexion as a result of recurrent hemorrhages which was resistant to treatment and consequently secondary developed degenerative joint disease. The patient had severe pain and deteriorating difficulty in the walking.
The patient was admitted to orthopedics clinic with these complaints, and diagnosed with left knee hemophilic arthropathy and factor replacement therapy was applied by a specialist in hematology. Then bleeding parameters had been checked, while left knees in the supine position, by entering the knee through the am-al portals with tourniquet, adhesions were attempted to open. Suprapatellar pouch had been opened, and only 10° of joint flexion could be provided and operation had been terminated due to planning of open surgery. After the patient had been stabilized the patient was referred to our clinic with the aim of rehabilitation. When we accepted the department, patient's left knee was in extension position and flexion was 10 degrees. The patient's patellar movements severely restricted and painfull.
The soft-tissue ultrasound was applied to the patient who described pain in both hips, and heterogeneous muscle plans and fluid levels between muscles around the left hip joint were observed (hemorrhage?). In addition, tensile tests were positive in the right sacroiliac joint. Morning stiffness lasted for 10 minutes. Family history and system background were unremarkable and other system examinations were normal, the lumbar and dorsal schober were normal. Chest expansion, occiput-wall distance, hand-ground distance was within normal limits. Other joint examinations were normal. Neurological examination was normal.
Routine blood, biochemistry, protein electrophoresis and urine tests were normal in the laboratory examinations. Erythrocyte sedimentation rate and CRP were normal. Brucella and salmonella serological tests, urine, blood and throat cultures were negative. Mycoplasma hominis, mycoplasma genitalium, ureoplasma ureolyticum, chlamydia trachomatis, and neisseria gonerhea were negative in urethral smear. Negative HLA-B27 and the PPD of 8 mm were detected and acid-resistant bacteria in sputum and sputum cultures were negative. Chest X-ray was normal. Lumbosacral radiography was unremarkable except for decreased lordosis. Arthropatic changes was observed in left knee radiograph (Fig. 1). Irregularity of the both sacroiliac joints was observed in private sacroiliac radiograph (Fig. 2) and MRI examination of the sacroiliac joints was performed. MRI of sacroiliac joints was considered as the right sacroiliitis because of irregularity in both sacroiliac joints and the signal decreased in T1 and increased in T2-weighted series in the right sacroiliac joint (Fig. 3, 4). paracetamol 2 gr/daily po was started for pain relief and after application of TENS and superficial heat therapy to the knee, range of motion and stretching exercises were performed.
 Click for large image | Figure 1. Arthropatic changes were observed in left knee radiograph. |
 Click for large image | Figure 2. Sclerosis and irregularity of both sacroiliac joints in x-ray. |
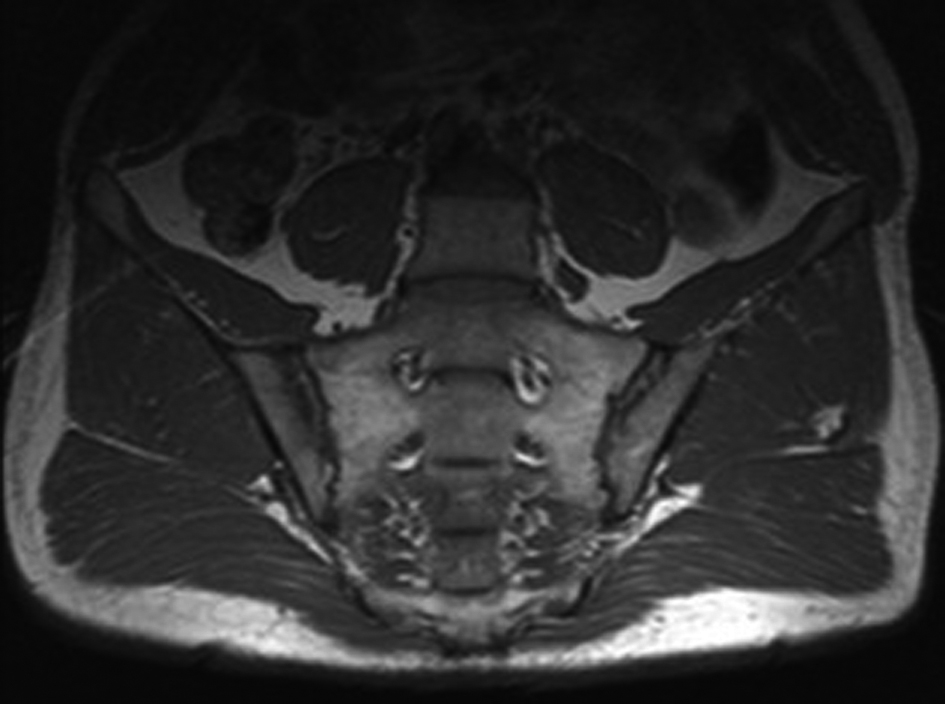 Click for large image | Figure 3. Hypointensity of add a neighboring section of the right iliac bone in MRI of the sacroiliac joint (T1 image). |
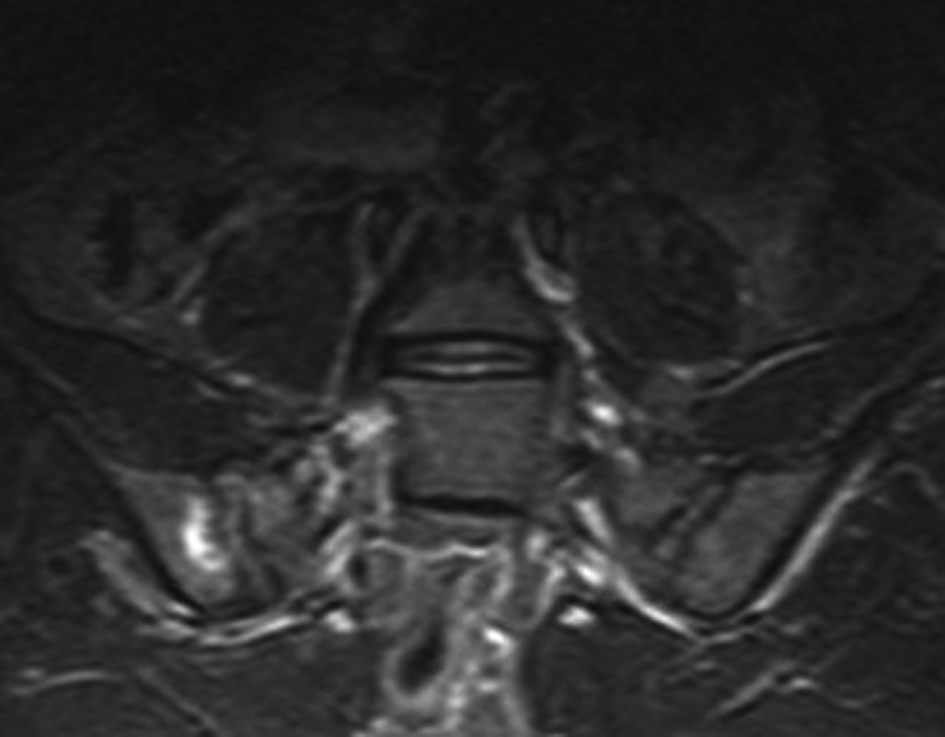 Click for large image | Figure 4. Hyperintensity of add a neighboring section of the right iliac bone in MRI of the sacroiliac joint (T2 image). |
Although the rehabilitation and treatment protocols have been continued up to three weeks, the patient did not achieve gains in knee flexion. Therefore the patient was given a home exercise program and referred to the further center for the surgical treatment of choice.
| Discussion | ▴Top |
Musculoskeletal bleeding is a common complication of hemophilia. Therefore, the hemophilic joint disease has been the subject of many reviews [3-10]. Hemarthrosis could be seen in almost all patients with severe hemophilia, and close to half of patients with mild to moderate disease activity [11]. Repeated hemarthrosis may begin at an early age, but occurs more often in children who started to walk. It can affect many joints. However, respectively, knee, elbow and ankle are more common affected [1]. Acute hemarthrosis causes chronic synovitis and consequently degenerative arthritis.
In our patient, there had been painful swelling in both knees since the age of 10, but hemophilia and hemophilic arthropathy had been diagnosed after 5 years of these complaints. Delay in diagnosis and treatment of our patient has lead to severe degenerative changes and loss of function in bilateral knees. In addition, right sacroiliitis was detected with MRI imaging and upon examination of the patient who described pain in both hips. As well as, areas of bleeding in the muscles of the left hip were detected by ultrasonography. The patient was examined in detail in terms of inflammatory rheumatic diseases. Morning stiffness, small joint involvement, inflammatory back pain, chest pain, alternating gluteal pain, uveitis, enthesitis, urethritis, conjunctivitis, diarrhea, constipation, psoriatic rash, acne, pustulosis, hyperostosis, oral aphthae, genital ulceration, urethritis, conjunctivitis were not detected in the patient. Necessary laboratory tests for the differential diagnosis of sacroiliitis (c-reactive protein, erytrosit sedimentation rate, complete blood count, urin tests, Rheumatoid factor, anti-CCP and HLA-B27, Brucella tube agglutination test, bacteriological and viral tests, PPD, parathyroid hormone) and imaging investigations (chest X-ray, sacroiliac x-ray and MRI) were performed. Thus, diseases which may cause sacroiliitis such as AS, chronic inflammatory bowel disease, psoriasis, tuberculosis, reactive arthritis, sarcoidosis, hyperparathyroidism were excluded. Thus, the current involvement of the sacroiliac joint was concluded to be hemophilic.
Hemophilic arthropathy occurs in the synovial joints and more often in the joints which exposed to injury. Sacroiliac joint is also a synovial joint in the front and 2/3 of lower part. However, frequent exposure to major trauma is uncommon. Intra-articular bleeding in patients with hemophilia may also occur due to minor trauma. More advanced degree of joint deformations in hemophilia occur in childhood. The reasons for this may be that the children could not protect from traumas themselves adequately and do not limit physical activities due to excessive interest of whom to play. However, previous reports on tendency to store iron in growing chondrocytes in animals suggest that this situation may also play an important role in the early stage of joint destruction in hemophilic children [12]. When background of our patient was queried, a trauma to the sacroiliac joint region was not identified. Considering for this case, toilet habits (Squatting on his knees), and especially the habit of sitting cross-legged in establishing both the knee in his daily life, spontaneous bleeding might occur depending on the strain of sacroiliac joint.
As a result, all the joints should be examined in detail in patients with hemophilic arthropathy. Especially in patients who admitted because of hip pain, hip and sacroiliac joint involvement together with soft tissue involvement should be considered.
| References | ▴Top |
- Rodriguez-Merchan EC. Musculoskeletal complications of hemophilia. HSS J. 2010;6(1):37-42.
doi pubmed - Madhok R, York J, Sturrock RD. Haemophilic arthritis. Ann Rheum Dis. 1991;50(8):588-591.
doi pubmed - Llinas A. Haemophilic arthropathy. Haemophilia. 2010;16 Suppl 5:121.
- Solimeno L, Goddard N, Pasta G, Mohanty S, Mortazavi S, Pacheco L, Sohail T, et al. Management of arthrofibrosis in haemophilic arthropathy. Haemophilia. 2010;16 Suppl 5:115-120.
- Roosendaal G, Jansen NW, Schutgens R, Lafeber FP. Haemophilic arthropathy: the importance of the earliest haemarthroses and consequences for treatment. Haemophilia. 2008;14 Suppl 6:4-10.
- Bossard D, Carrillon Y, Stieltjes N, Larbre JP, Laurian Y, Molina V, Dirat G. Management of haemophilic arthropathy. Haemophilia. 2008;14 Suppl 4:11-19.
- Lafeber FP, Miossec P, Valentino LA. Physiopathology of haemophilic arthropathy. Haemophilia. 2008;14 Suppl 4:3-9.
- Negrier C, Goudemand J, Lambert T. Haemophilic arthropathy from A to Z. Introduction. Haemophilia. 2008;14 Suppl 4:1-2.
- Mejia-Carvajal C, Hakobyan N, Enockson C, Valentino LA. The impact of joint bleeding and synovitis on physical ability and joint function in a murine model of haemophilic synovitis. Haemophilia. 2008;14(1):119-126.
pubmed - Rodriguez-Merchan EC. Common orthopaedic problems in haemophilia. Haemophilia. 1999;5 Suppl 1:53-60.
- Steven MM, Yogarajah S, Madhok R, Forbes CD, Sturrock RD. Hemophilic arthritis. Q J Med 1986;58:181-97.
pubmed - Fabry G. Early biochemical and histological findings in experimental hemarthrosis in dogs. Arch Orthop Trauma Surg. 1982;100(3):167-173.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Hematology is published by Elmer Press Inc.